Case of the Week #649
Femicare, Center of prenatal ultrasonographic diagnostics, Martin, Slovakia
A 26-year-old primigravida with an unremarkable medical history underwent a fetal ultrasound examination at 22 weeks gestation. The following images and video clips demonstrate the findings.

View the Answer Hide the Answer
Answer
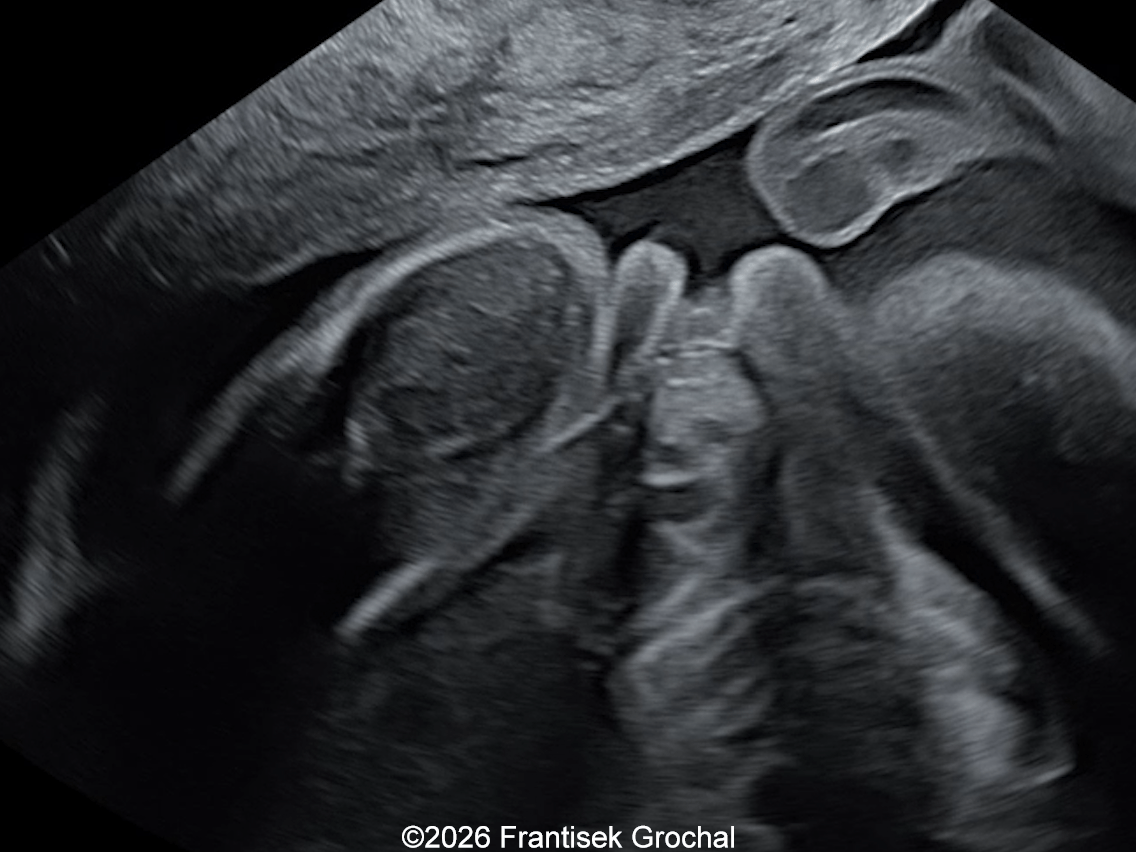
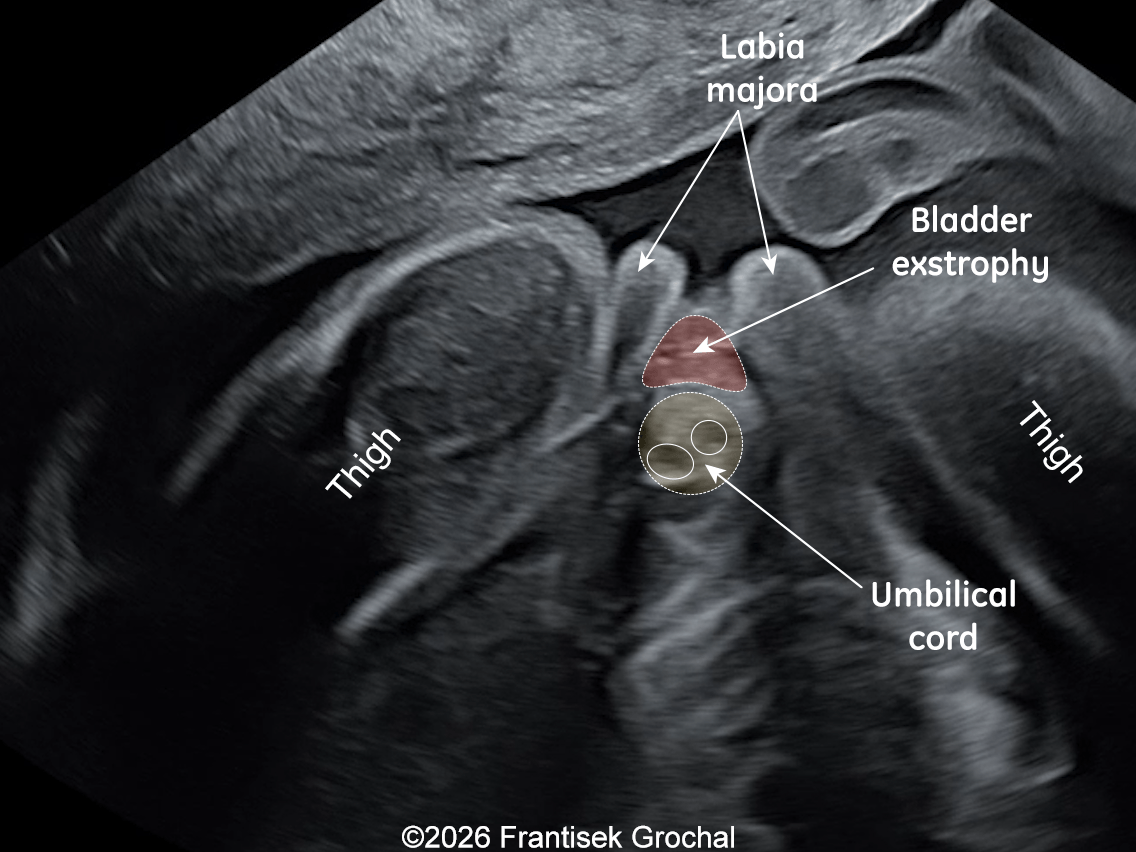
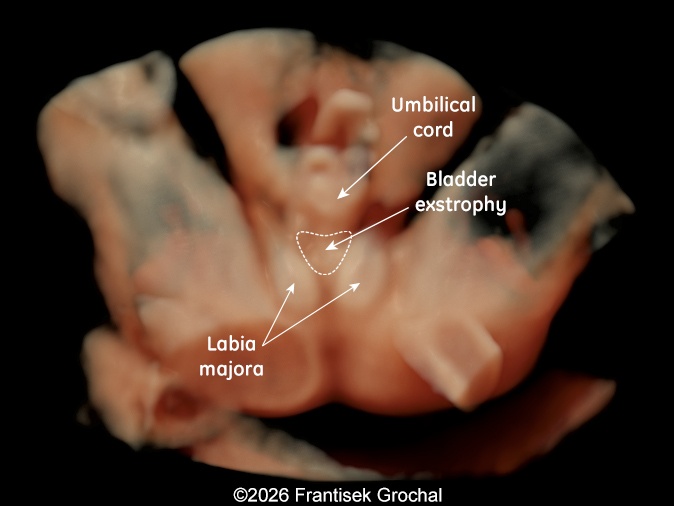
We present a case of bladder exstrophy seen in a female fetus at 22 weeks gestation.
Our ultrasound revealed nonvisualization of the urinary bladder with low umbilical cord insertion, normal kidneys and amniotic fluid volume. These findings suggested the diagnosis of classical bladder exstrophy. After counseling, the parents opted for the termination of the pregnancy.
Discussion
The exstrophy–epispadias complex is a spectrum of congenital anomalies that ranges in severity from isolated epispadias, to classic bladder exstrophy, to the most severe form, cloacal exstrophy, often referred to as OEIS complex (Omphalocele, Exstrophy of the cloaca, Imperforate anus, and Spinal defects) as it is associated with omphalocele, imperforate anus, and vertebral defects [1,2]. These conditions are caused by defective midline closure of the lower abdominal wall with abnormal partitioning of the cloacal membrane preventing mesodermal fusion [1,3]. In classic bladder exstrophy, the posterior bladder wall is exposed externally and is frequently associated with genital and pelvic skeletal abnormalities. The estimated prevalence is 1 in 30,000 to 50,000 births [1,4].
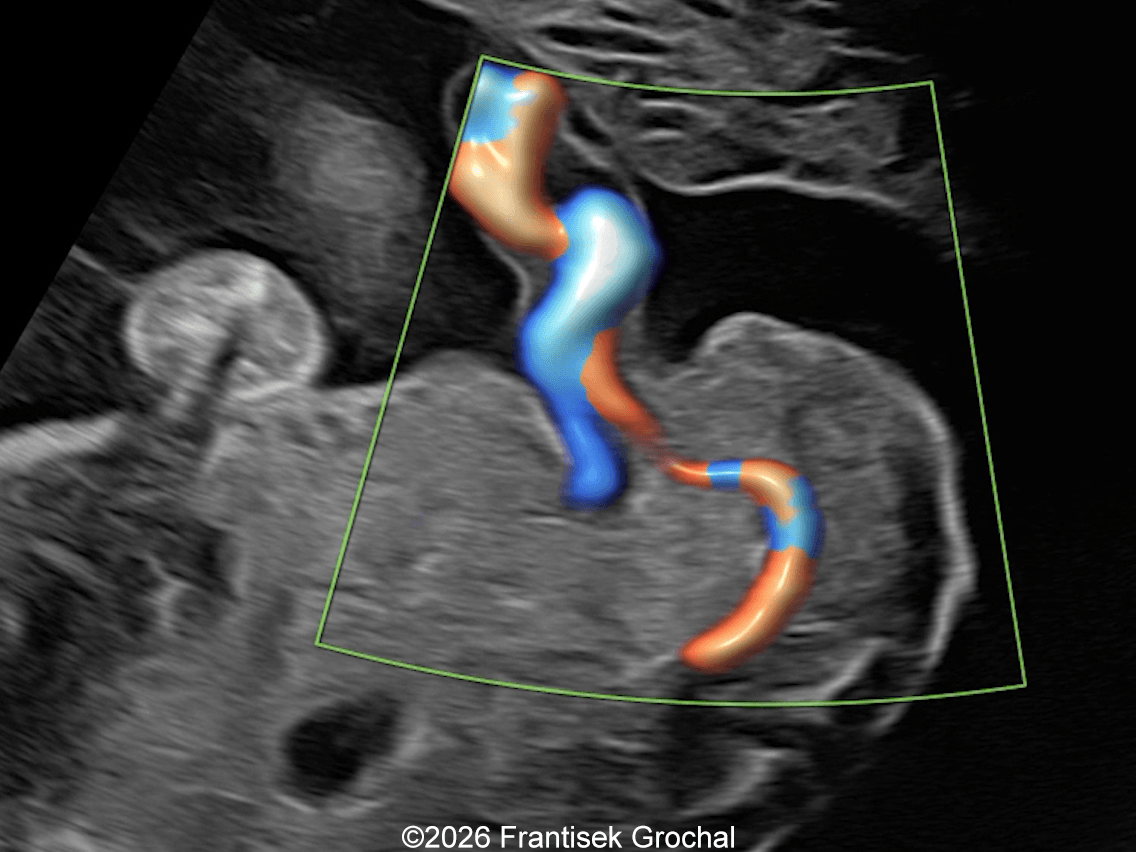
Prenatal diagnosis is based on persistent non-visualization of the fetal bladder despite normal kidneys, normal amniotic fluid volume, and adequate time for bladder filling (30-60 minutes). Additional sonographic findings include protrusion of a solid mass between the two umbilical arteries, low umbilical cord insertion, splayed iliac bones or pubic diastasis, and abnormal external genitalia [2-4]. The abdominal wall mass is thought to represent severe bladder hypoplasia and squamous metaplasia of the remaining mucosa [4]. Recognition of these features allows differentiation from omphalocele, gastroschisis, and cloacal exstrophy, though prenatal diagnosis only occurs in approximately 46% of fetuses with bladder exstrophy [3].
Early diagnosis is essential for parental counseling, as postnatal management requires complex staged reconstructive surgery and may be associated with long-term urinary and functional complications [1,3,5]. A staged approach to repair of bladder exstrophy includes reconstruction of the bladder and primary closure of the abdominal wall at birth. At 12–18 months of age, surgery involves repair of the epispadias with corporeal lengthening, dorsal chordee release and urethroplasty in male patients, and vulvoplasty with clitoroplasty in female patients. Operations for urinary continence including bladder neck reconstruction as well as antireflux procedures are performed between 4–8 years of age [1,3]. After surgical correction, urinary continence can be achieved in 90% of cases. Fertility in females is normal, while male patients often require assisted reproductive technologies to father a child [1,2]. Additionally, the patients with bladder exstrophy are at increased risk of developing cancer [5]. These considerations may influence parental decision-making, though pregnancy termination is not routinely advocated [1].
References
- Ebert AK, Reutter H, Ludwig M, et al. The exstrophy-epispadias complex. Orphanet J Rare Dis. 2009 Oct 30:4:23.
- Mallmann MR, Mack-Detlefsen B, Reutter H, et al. Isolated bladder exstrophy in prenatal diagnosis. Arch Gynecol Obstet. 2019 Aug;300(2):355-363.
- Hirsch AM, Morrill CC, Haffar A, et al. Optimizing prenatal diagnosis and referral of classic bladder exstrophy: Lessons from a single-institution experience. J Pediatr Urol. 2024 Aug;20(4):619-627.
- Lee E-H, Shim JY. New sonographic finding for the prenatal diagnosis of bladder exstrophy: a case report. Ultrasound Obstet Gynecol. 2003 May;21(5):498-500.
- Woodhouse CRJ, North AC, Gearhart JP. Standing the test of time: long-term outcome of reconstruction of the exstrophy bladder. World J Urol. 2006 Aug;24(3):244-
Discussion Board
Winners

francesca ullo Italy Physician
Seadet Zeynalova Azerbaijan Physician
Pawel Swietlicki Poland Physician

Andrii Averianov Ukraine Physician

Alexandr Krasnov Ukraine Physician

Mayank Chowdhury India Physician

Nutan Thakur India Physician

Vladimir Lemaire United States Physician
Shilpen Gondalia India Physician
Ivan Ivanov Russian Federation Physician
Rati Chadha United States

carlos lopez Venezuela Physician
Miğraci Tosun Turkey Physician
Maneet Kaur United States
Yana Brudner Israel Physician

CHEN YANG China Physician
Amparo Gimeno Spain Physician

Elena Andreeva Russian Federation Physician

ALBANA CEREKJA Italy Physician
Eti Zetounie Israel Sonographer

Murat Cagan Turkey Physician
rahous karim United States
ANA PAULA PASSOS Brazil Physician

Fatih Akkuş Turkey Physician

Ionut Valcea Romania Physician

Hien Nguyen Van Viet Nam Physician

Almaz Kinzyabulatov Russian Federation Physician
Daniil Gagaev Russian Federation Physician
Anette Beverdam Netherlands Sonographer

Annette Reuss Germany Physician
Seadet Zeynalova Azerbaijan Physician
Vu The Anh Viet Nam Physician
CHERYL TURNER United States Sonographer

YULIA VISHNEVSKAYA Russian Federation Physician

Nguyen Xuan Cong Viet Nam Physician

Perrine Riou-Kerangal French Polynesia Sage-femme échographiste
shay kevorkian Israel Physician

Ismail Guzelmansur Turkey Physician
Laura Wharton United Kingdom Physician
Un Wong Australia Sonographer
Rohit Sanghani India Physician
Joanna Głowska-Ciemny Poland Physician

Nguyễn Lê Hoàng Viet Nam Physician

Tetiana Ishchenko Ukraine Physician
Debbie Flores United States Sonographer

Hana Habanova Slovakia Physician
Caroline Gregoir Belgium Physician

Petra Tallova Slovakia Physician

Ashlea Hardin United States Sonographer
Robert Brawura-Biskupski-Samaha Poland Physician
LEVENT KANDEMİR Turkey Physician
Ayse Ceren Duymus Turkey Physician

Viktorya Mkrtchyan Armenia Physician
ZHANNA Kurmangaliyeva Kazakhstan Physician
Natalia Omelyanovich Russian Federation Physician

Olga Gundareva Russian Federation Physician

Sergey Shumakov Russian Federation Physician
Carmie Cee Australia Physician
ANDRES ARENCIBIA MOLINA United States Physician
burcu gedik Turkey Physician
Guillermo Fernández Lizana Spain Physician
Sulueti Bauleka New Zealand Sonographer
Anne Janke Germany Physician
Simen Vergote Canada Physician
MISCHEL BARTIE United States Sonographer

Mert Eyupoglu Turkey Physician

Gulten Rafibeyli Azerbaijan Physician

Ayten Sadigova Azerbaijan Physician

Gulsum Mammadova Azerbaijan Physician
Aynur Garibova Azerbaijan Physician
Ulviyya Jafarova Azerbaijan Physician
Elnara Suleymanova Azerbaijan Physician

Nataliia Antonenko Ukraine Physician
Tenzen Youndan India Physician
Eva Kornanova Slovakia Physician