Case of the Week #619
(1) Department of Genetics, Polish Mother's Memorial Hospital, Lodz, Poland; (2) UCSF Health, San Francisco, California, USA
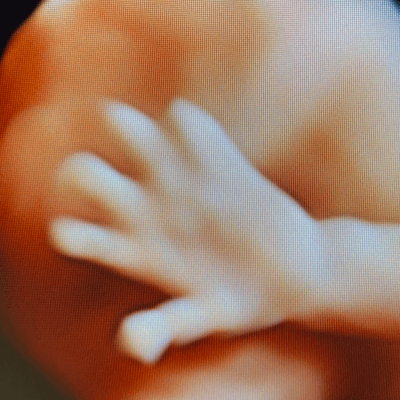
33-year-old primigravida with non-contributive anamnesis presented at 20 weeks for an anomaly scan. The findings are presented in the video. There were no other abnormalities noted by the operator.
View the Answer Hide the Answer
Answer
We present a case of Congenital aural atresia with unilateral microtia and ipsilateral hypoplasia of the tympanic ring.

The findings were confirmed after birth. Additionally, the right ear canal was found to be atretic and the child had conductive hearing loss. Consent was obtained from the parents to publish the child's photos.



Discussion
Microtia is a spectrum of congenital anomalies of the auricle that range from mild structural abnormalities to complete absence of the ear occurring in 2.9 to 3.8 per 10,000 births [1-3]. Approximately 90% of individuals with microtia experience conductive hearing loss on the affected side [4]. Microtia is unilateral in 77–97% of cases, affecting the right ear in 68% of individuals, and occurring more commonly in males [3,5-6]. Microtia may occur as an isolated condition, though in 27-55% of cases are associated with other anomalies [3,5-6]. In a study reviewing 672 patients with microtia, 40% had malformations of the ear, face, and neck, 35% of the musculoskeletal system, and 11% of the cardiovascular system [5]. The most common anomalies associated with microtia include oral clefts, facial asymmetry, macrostomia, microphthalmia, vertebral anomalies, polydactyly and cardiac defects such as atrial septal defect and ventricular septal defect [4,5]. Associated syndromes include Crouzon syndrome, Treacher-Collins syndrome, Goldenhar syndrome and Pierre-Robin sequence [7] while chromosomal anomalies occur in 23% and include trisomies 18, 13, 21 as well as 22q11 microdeletion [6]. Single gene mutations are associated with microtia in syndromic and familial cases, whereas multifactorial or polygenic causes are more probable in sporadic cases [4].
The auricle begins its development during the fifth week of embryogenesis from several protuberances in the first and second pharyngeal arches known as the auricular hillocks. The auditory canal and tympanic membrane are derived from ectoderm of the pharyngeal cleft that separates the first and second pharyngeal arches [4]. At 20 weeks of gestation, both the morphology of the auricle [6] and the size of the tympanic ring [8] is similar to that of adults. The tympanic ring is a C-shaped bone structure that forms during embryogenesis and is subsequently integrated into the temporal bone [8].
Congenital aural atresia is an ear deformity occurring in 0.6 to 1.3 in 10,000 births [1,9] and resulting from tympanic ring hypoplasia or aplasia with subsequent external auditory meatus atresia and congenital conductive hearing loss [7]. It is often associated with malformations of the auricle such as microtia. The differential diagnosis of congenital aural atresia includes Treacher Collins syndrome as well as oculo-auriculo-vertebral spectrum. Treacher Collins syndrome is a rare genetic disorder caused by a gene mutation mapped to chromosome 5q and characterized by craniofacial abnormalities including micro or retrognathia, hypoplasia of the facial bones, cleft palate, abnormalities of the pinnae or low-set ears, macrosomia and deafness [10]. Oculo-auriculo-vertebral spectrum, is characterized by facial asymmetry, microtia, ear and facial tags, epibulbar dermoids, microphthalmia, and macrostomia [4].
There is a strong association between aplasia and hypoplasia of the tympanic ring, microtia, and congenital aural atresia, making this ring a sensitive marker of congenital hearing loss [8,11]. Leibovitz et al first reported the normal development of the fetal tympanic rings by prenatal ultrasound. On ultrasound, the fetal tympanic ring is demonstrated by aligning the imaging plane on the inferolateral surface of the petrous part of the temporal bone where a circular echogenic contour is seen in the oblique axial plane [7]. Unlike the adult ear, the tympanic rings in the fetus are located inferiorly and obliquely relative to the auricle. Anatomically, the tympanic ring is an incomplete bony annulet with a small deficient segment on its lateral margin corresponding to the pars flaccida of the tympanic membrane. Leibovitz et al found that the tympanic ring is identified in 90% of fetuses at 16 weeks and 80% of fetuses at 23 weeks [7]. They hypothesized that difficult visualization at the earlier gestational ages was due to a small tympanic ring with incomplete ossification, whereas at later gestational ages, it was due to ossification of the surrounding petrous part of the temporal bone [7]. They imaged the tympanic rings of fetuses with microtia and found that these tympanic rings were smaller than fetuses with normal auditory development.
MRI has been reported to visualize the middle ear structures in the fetus. The tympanic cavity appears T2 hyperintense due to its fluid content while the ossicles within the tympanic cavity are T2 hypointense. Katorza et al present two fetuses with ear deformities, one case of Treacher Collin syndrome and the second with oculo-auriculo-vertebral spectrum. Both cases demonstrated poor visualization of the tympanic cavity and nonvisualization of the hypointense ossicles on fetal MRI which was consistent with middle ear hypoplasia [10].
In conclusion, abnormalities of the ear seen by ultrasound should prompt an evaluation of the tympanic ring by ultrasound or tympanic cavity and ossicles by MRI, which may help diagnose congenital hearing loss. Additionally, other anomalies of the face, musculoskeletal system and heart should be assessed in order to diagnose associated syndromes such as Treacher Collin syndrome and oculo-auriculo-vertebral spectrum. This could provide valuable information for patient counseling.
References
[1] Shaw GM, Carmichael SL, Kaidarova Z, et al. Epidemiologic characteristics of anotia and microtia in California, 1989-1997. Birth Defects Res A Clin Mol Teratol. 2004 Jul;70(7):472-5.
[2] Forrester MB, Merz RD. Descriptive epidemiology of anotia and microtia, Hawaii, 1986-2002. Congenit Anom (Kyoto). 2005 Dec;45(4):119-24
[3] Canfield MA, Langlois PH, Nguyen LM et al. Epidemiologic features and clinical subgroups of anotia/microtia in Texas. Birth Defects Res A Clin Mol Teratol. 2009 Nov;85(11):905-13.
[4] Luquetti DV, Heike CL, Hing AV et al. Microtia: epidemiology and genetics. Am J Med Genet A. 2012 Jan;158A(1):124-39.
[5] Zhang Y, Jiang H, Yang Q et al. Microtia in a Chinese Specialty Clinic Population: Clinical Heterogeneity and Associated Congenital Anomalies. Plast Reconstr Surg. 2018 Dec;142(6):892e-903e.
[6] Qiu J, Ru Y, Gao Y, et al. Experience in prenatal ultrasound diagnosis of fetal microtia and associated abnormalities. Front Med (Lausanne). 2023 Jul 11;10:1119191.
[7] Leibovitz Z, Egenburg S, M Bronshtein M, et al. Sonographic imaging of fetal tympanic rings. Ultrasound Obstet Gynecol. 2013 Nov;42(5):536-44.
[8] Nuñez-Castruita A, López-Serna N. Prenatal development of the human tympanic ring: a morphometric study with clinical correlations. Surg Radiol Anat. 2021 Jul;43(7):1187-1194.
[9] Zernotti ME, Curet CA, Cortasa S, et al. Congenital Aural Atresia prevalence in the Argentinian population. Acta Otorrinolaringol Esp (Engl Ed). 2019 Jan-Feb;70(1):32-35.
[10] Katorza E, Nahama-Allouche C, Castaigne V, et al. Prenatal evaluation of the middle ear and diagnosis of middle ear hypoplasia using MRI. Pediatr Radiol. 2011 May;41(5):652-7.
[11] Chen K, Liu L, Shi R, et al. Correlation among external auditory canal anomaly, temporal bone malformation, and hearing levels in patients with microtia. Ear Nose Throat J. 2017 Jun;96(6):210-217.
Discussion Board
Winners

Zhanna Bondarchuk Ukraine Physician

Dianna Heidinger United States Sonographer

Javier Cortejoso Spain Physician
paola quaresima Italy Physician

Pawel Swietlicki Poland Physician

Alexandr Krasnov Ukraine Physician

Mayank Chowdhury India Physician
Ivan Ivanov Russian Federation Physician

Aysegul Ozel Turkey Physician
Irvin Jacob Vélez Machorro Mexico Physician
Anita Silber Israel Physician
Kimberly Delaney United States Sonographer

ALBANA CEREKJA Italy Physician
Bridget Sparks New Zealand Sonographer
Bailey Brown New Zealand Sonographer

Deval Shah India Physician
ALPESH PANCHOLI United States

Murat Cagan Turkey Physician
Eslam Adel ammar Egypt Physician

Loai Said Palestinian Territory, Occupied Physician

Ionut Valcea Romania Physician

Seda Cam Turkey Physician

Kareem Haloub Australia Physician
Subapriya Kandasamy India Physician

abdullah sarıyıldırım Turkey Physician
Ann-Christin Dr. Sönnichsen Germany Physician
Annette Reuss Germany Physician
Jay Vaishnav India Physician
CHERYL TURNER United States Sonographer

Perrine Riou-Kerangal French Polynesia Sage-femme échographiste
Mary Jones United States Sonographer

Samir Arus Brazil Physician

Veronika Bartkovjaková Slovakia Physician

Dr.Umashankar Kawlas India Physician
Rohit Sanghani India Physician
Rupal Sasani India Physician

Le Tien Dung Viet Nam Physician

Tetiana Ishchenko Ukraine Physician

Le Duc Viet Nam Physician
Dr Dhara patel India Physician

Joanne Maloney United States Sonographer

Dr Mayur C Trivedi India Physician
Gnanasekar Periyasamy India Physician
Navya Sri Mopada India Physician
Jagdish Suthar India Physician
Petra Tallova Slovakia Physician
Sana MV India Physician
Hân Đỗ Viet Nam Physician

CARLOS JOSE PIÑA VILLEGAS Peru Physician
Clary Gomerez United States Sonographer
sugunadevi Viswanathan India Physician

Kurmanzhan Balmukhambetova Kazakhstan Physician

Ali Ozgur Ersoy Turkey Physician
Gökçen Örgül Turkey Physician