Case of the Week #584
Division of Maternal Fetal Medicine, Department of Obstetrics and Gynecology, and Department of Radiology, University of New Mexico, Albuquerque, NM
26-year-old G2 P1001 was seen at 26 weeks gestation in the perinatal outreach clinic for suspected brain anomalies. The patient has history of obesity, alcohol abuse disorder and latent syphilis of unknown duration which was treated with Benzathine Penicillin G weekly for 3 weeks.

View the Answer Hide the Answer
Answer
We present a case of PHACE syndrome.
Our ultrasound revealed the following:
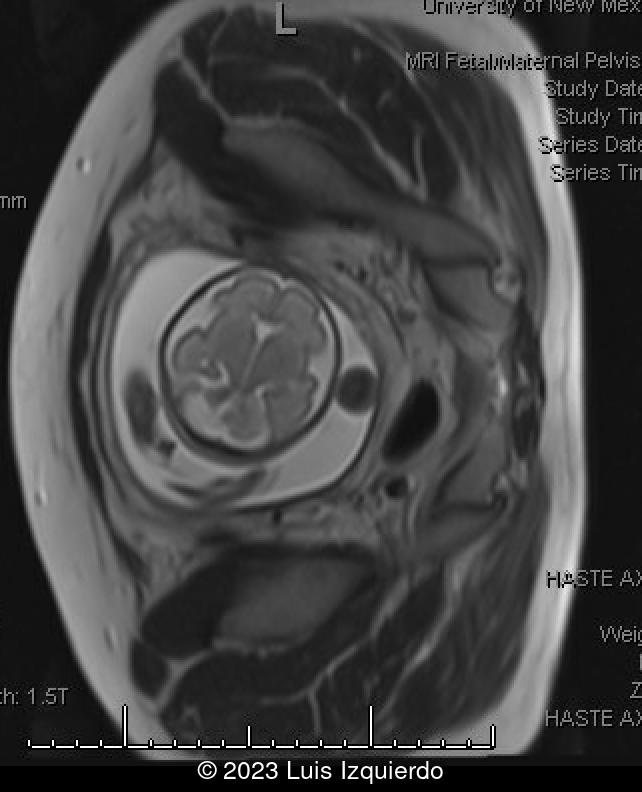
- Image 1: Axial view of the fetal brain at the level of the transverse cerebellar diameter. Note that the inferior cerebellar hemisphere is smaller than the one insonated superiorly.
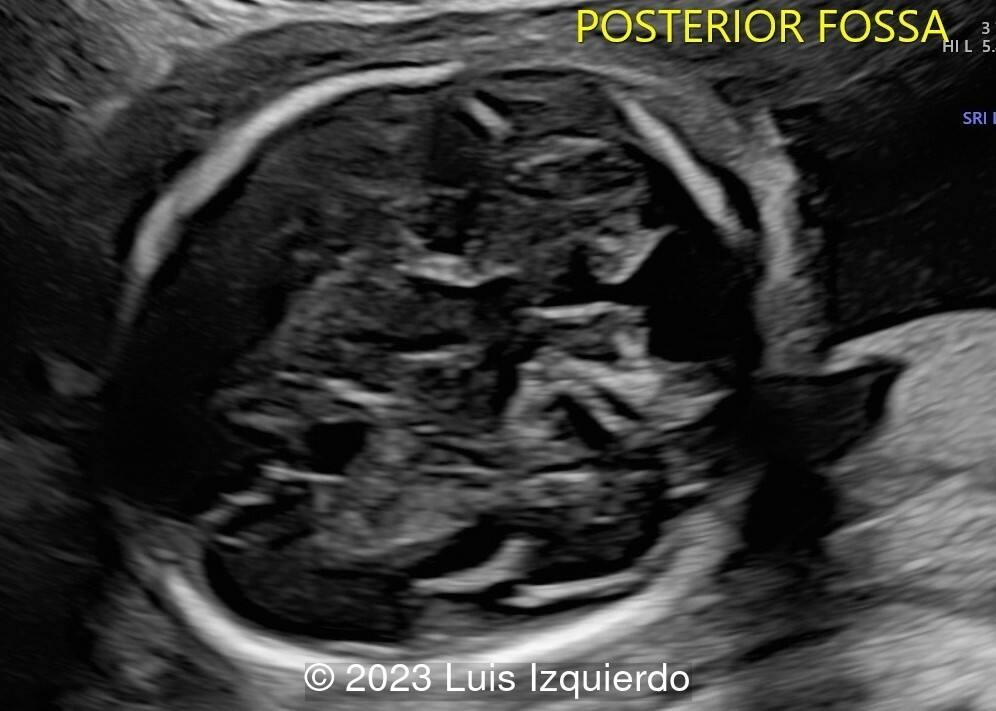
- Image 2: Axial image of the posterior fossa demonstrating hypoplasia of the cerebellar hemisphere.
- Video 1: Video demonstrating both axial planes of the posterior fossa.
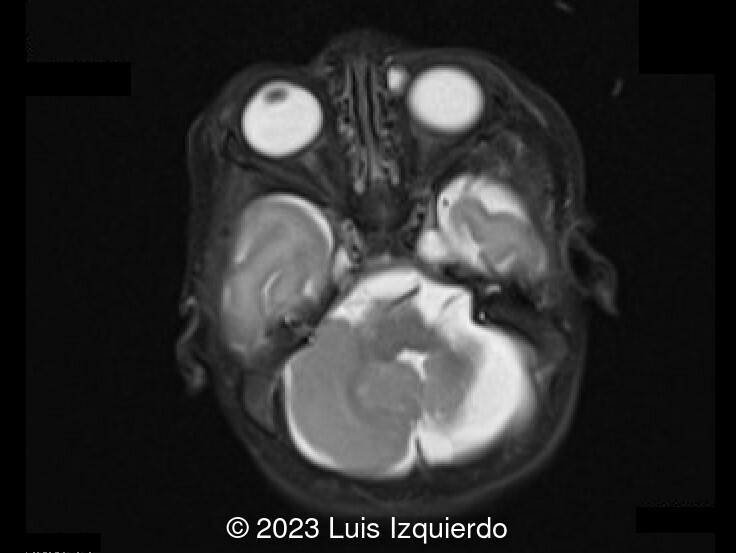
- Image 3: Fetal MRI shows a severely hypoplastic left cerebellar hemisphere with mild hypoplasia of the vermis, communication of the fourth ventricle with the cisterna magna, and mildly increased tegmentovermian angle
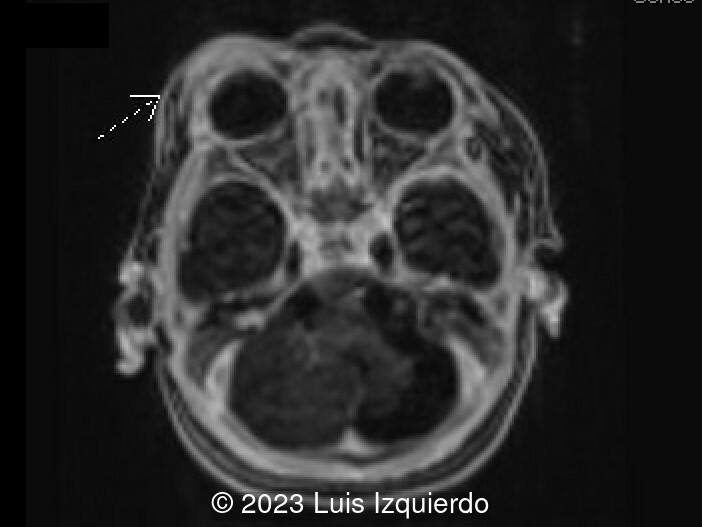
Postnatal MRI was obtained and confirmed the prenatal findings (Image 1) in addition to an enhancing, asymmetric ill-defined soft tissue lesion of the right peri/supraorbital soft tissues (Image 2), consistent with a hemangioma. MR angiogram (Image 3) demonstrates:
- Early bifurcation of the left external carotid and internal carotid arteries with focal tortuosity of the distal cervical left internal carotid artery.
- Left-sided carotid/basilar artery anastomosis via persistent trigeminal artery.
- Right internal carotid artery (ICA) terminates in the posterior cerebral artery without continuation of the distal right ICA, potentially also reflecting persistent trigeminal artery.
- Right middle cerebral artery is supplied via anterior communicating artery from the left-sided anterior circulation.

Discussion
PHACE syndrome describes a rare neuro-cutaneous syndrome characterized by Posterior fossa malformations, Hemangiomas of the face, Arterial anomalies, Coarctation of the aorta and cardiac defects, and Eye abnormalities [1]. The classical phenotype is the presence of a large segmental facial hemangioma, which almost always becomes evident during the first weeks of life. Central nervous system (CNS) structural malformations and cerebrovascular anomalies are the most frequent extracutaneous manifestations, with an incidence of 45% and 35%, respectively [2]. CNS structural anomalies include cerebellar hypoplasia which affects 20% of patients, Dandy–Walker complex, vermian dysgenesis/agenesis, abnormalities of the fourth ventricle (mainly enlargement and/or communication with the cisterna magna), brainstem hypoplasia, cerebellar germinal matrix hemorrhage/siderosis, and Chiari I malformation [2]. Cerebrovascular abnormalities include hypoplasia or segmental agenesis of major cerebral arteries, persistence of embryonic vessels, arterial stenoses, and segmental elongation and dilatation of intracranial arteries [2]. In 2009, a consensus statement on diagnostic criteria for PHACE syndrome was published and defined both major and minor criteria in several organ systems including cerebrovascular, structural brain, cardiovascular, ocular, and ventral/midline. Definite PHACE requires the presence of a >5 cm segmental hemangioma on the face or scalp in addition to one major criterion or two minor criteria [3]. Malformations of the posterior fossa is considered a major diagnostic criterion, as well as anomalies of major cerebral arteries, aortic arch anomalies, ocular posterior segment anomalies, and sternal defects [1].
Prenatal diagnosis is rare and the detection of a posterior fossa malformation may be the first clue to the diagnosis of PHACE syndrome [1,4]. In 2014 Fernandez et al, reported the first case of prenatally suspected PHACE based on the association of unilateral cerebellar hypoplasia with microphthalmia [4]. Previously, several cases of PHACE were diagnosed postnatally with prenatal findings [5-7]. Fetal magnetic resonance imaging is critical in evaluating the posterior fossa [1,2,4]. In a review of 10 fetuses with unilateral cerebellar hypoplasia and postnatal diagnosis of PHACE, Leibovitz et al defined a "tilted telephone receiver sign" on the coronal plane through the upper vermis. This sign was absent in 11 fetuses without postnatal diagnosis of PHACE. MRI also demonstrated this finding: the affected hemisphere upwardly displaced by an ipsilateral posterior fossa cyst communicating with an asymmetrically distended 4th ventricle [2].
On the coronal plane, the "tilted telephone receiver sign" is described as:
- upward displaced unilateral hypoplastic cerebellar hemisphere
- asymmetric dilated 4th ventricle connected to as ipsilateral retrocerebellar cyst
- elongated oblique connection between the hemispheres formed upwardly rotated and deviated vermis merging with the contralateral cerebellar peduncle
The differential diagnosis for unilateral cerebellar hypoplasia can include ischemic or hemorrhagic insults, PHACE syndrome and congenital cytomegalovirus [8]. In addition to PHACE, unilateral cerebellar hypoplasia can be associated with syndromes such as Goldenhar, Aicardi, and Moebius [4]. Fetal karyotyping has been performed in cases with unilateral cerebellar hypoplasia, often with normal results.
The incidence of neurologic manifestations ranges from 50% to 90% when there is evidence of CNS or cerebrovascular anomalies [2], and can include neurodevelopmental delay, speech difficulties, seizures, and neurovascular complications such as severe headache and acute ischemic stroke [1,2].
References
[1] Sepulveda W, Sepulveda F. Fetal neuroimaging findings in PHACE syndrome: case report and review of the literature. J Matern Fetal Neonatal Med. 2022 Jul;35(14):2751-2758.
[2] Leibovitz Z, Guibaud L, Garel C, et al. The cerebellar "tilted telephone receiver sign" enables prenatal diagnosis of PHACES syndrome. Eur J Paediatr Neurol. 2018 Nov;22(6):900-909.
[3] Metry D, Heyer G, Hess C, et al. Consensus statement on diagnostic criteria for PHACE syndrome. Pediatrics. 2009;124(5):1447–1456.
[4] Fernández-Mayoralas DM, Recio-Rodríguez M, Fernández-Perrone AL, et al. In utero diagnosis of PHACE syndrome by fetal magnetic resonance imaging (MRI). J Child Neurol. 2014 Jan;29(1):118-21.
[5] Gonçalves LF, Grillo E. PHACES syndrome with cerebellar hemihypoplasia. TheFetus.net. https://thefetus.net/content/phaces-syndrome-with-cerebellar-hemihypoplasia. Publish date, 6/2002.
[6] Carles D, Pelluard F, Alberti EM, et al. Fetal presentation of PHACES syndrome. Am J Med Genet A. 2005 Jan 1;132A(1):110.
[7] Juan M, Pomar I, Tubau A, et al. Unilateral cerebellar hypoplasia:primary prenatal finding of Phaces syndrome, a case report (abstract). Ultrasound Obstet Gynecol. 2008;32:407
[8] Massoud M, Cagneaux C, Garel C, et al. Prenatal Unilateral Cerebellar Hypoplasia in a series of 26 cases: significance and implications of prenatal diagnosis. Ultrasound Obstet Gynecol. 2014 Oct;44(4):447-54.
Discussion Board
Winners

Javier Cortejoso Spain Physician

Umber Agarwal United Kingdom Maternal Fetal Medicine

Mayank Chowdhury India Physician

Nguyen Luân Viet Nam Physician
gholamreza azizi Iran, Islamic Republic of Physician

Ionut Valcea Romania Physician
Đặng Mai Quỳnh Viet Nam Physician
Annette Reuss Germany Physician

Mai Phương Viet Nam Physician