Case of the Week #562
Femicare, Center of prenatal ultrasonographic diagnostics, Martin, Slovakia
Posting Dates: June 30 - July 14, 2022
Reviewer: Sara Abdallah Salem
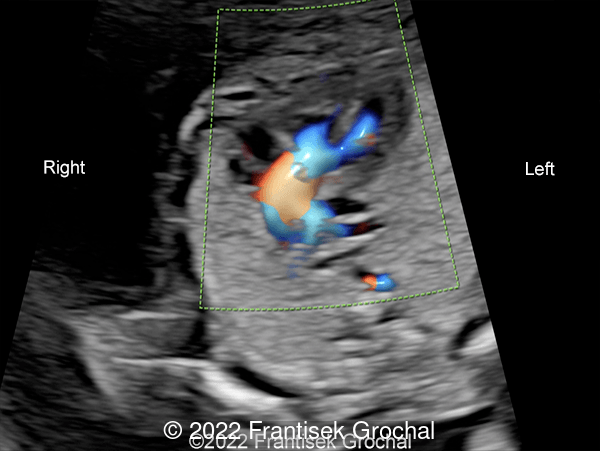
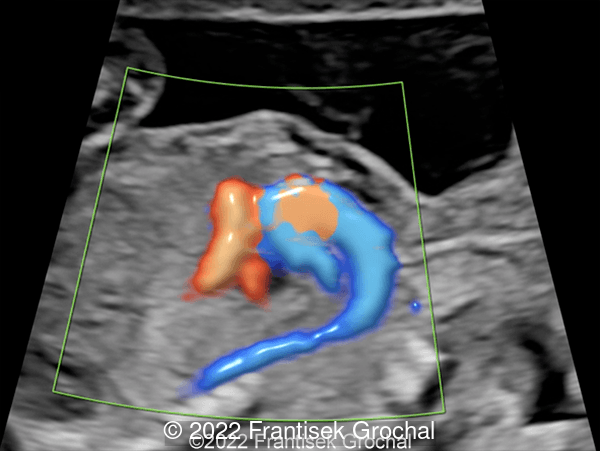
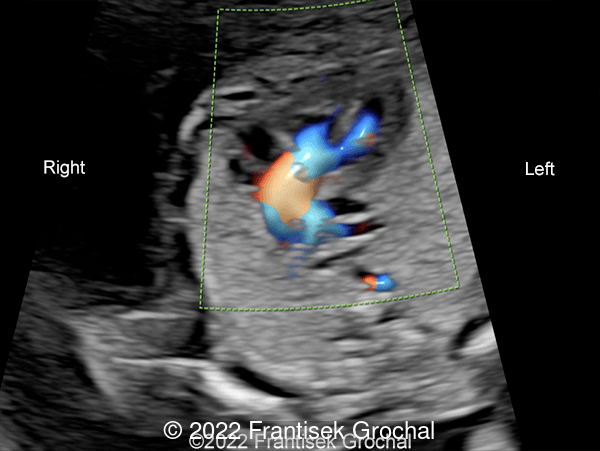
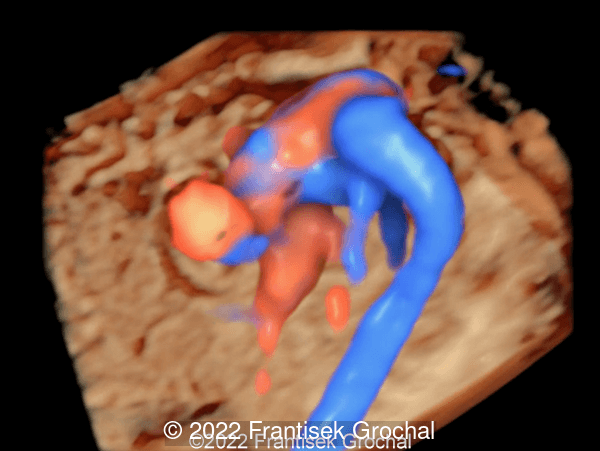
Case Report: A 24-year-old woman (G1P0) with non-contributive history was sent to our facility at 20 weeks of gestation. Our ultrasound examination revealed following findings. Please describe the cardiac anomaly.

View the Answer Hide the Answer
Answer
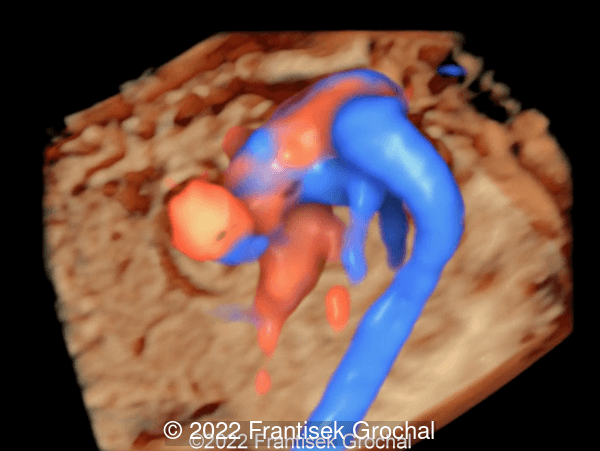
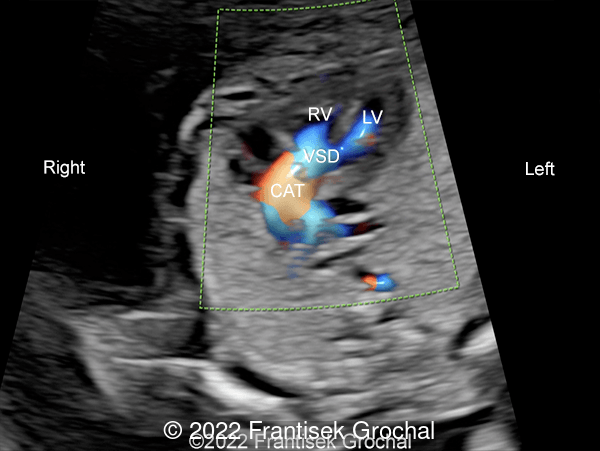
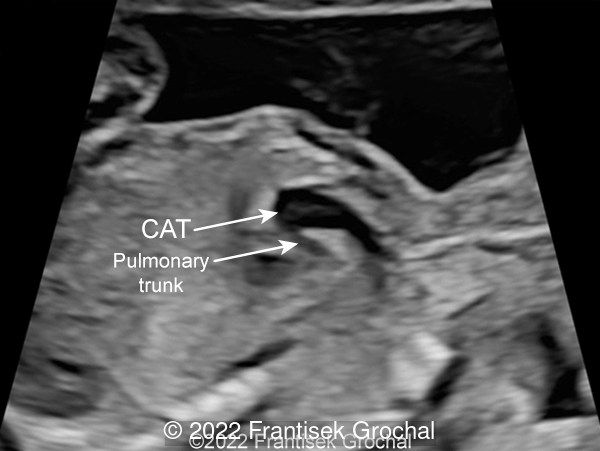
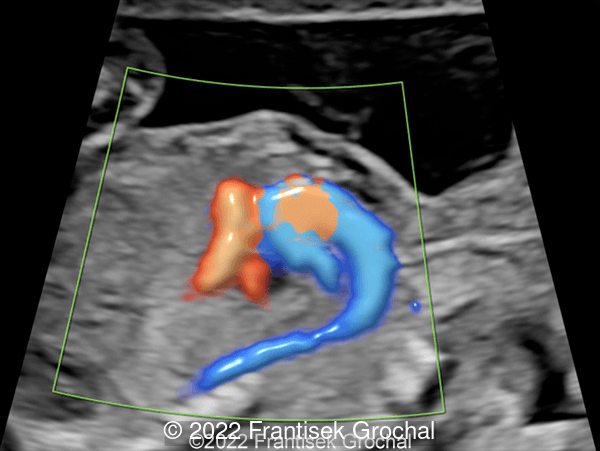
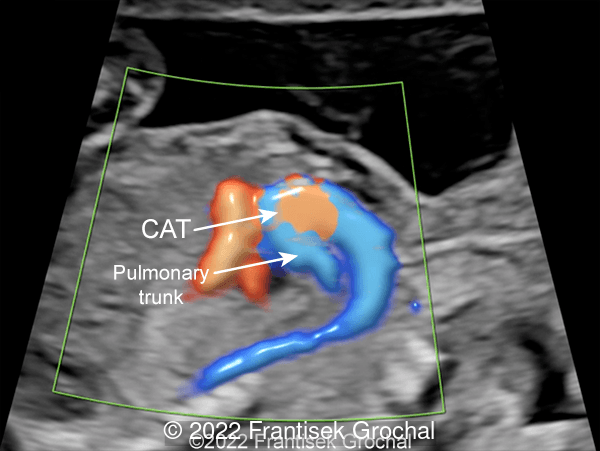
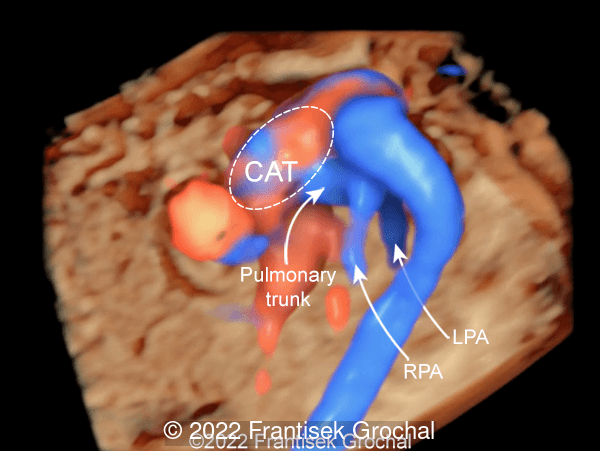
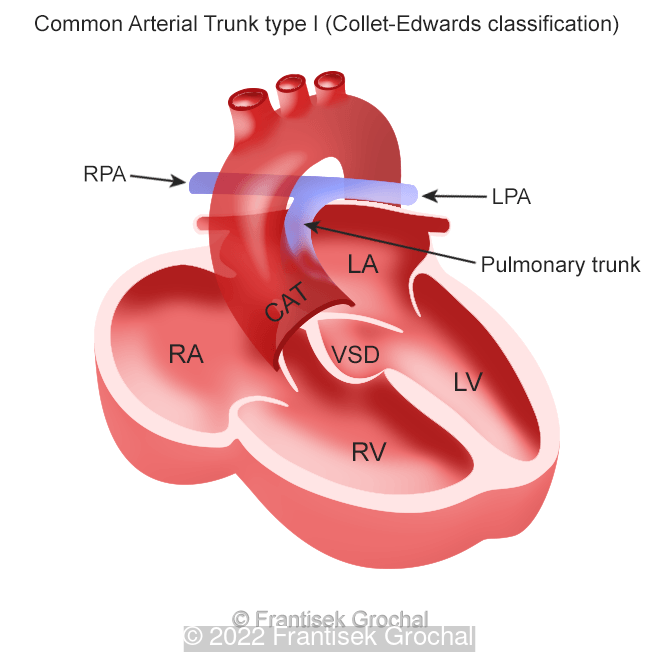
Our ultrasound examination revealed Common Arterial Trunk type I (Collet-Edwards classification) of the fetus. The parents opted for the termination of the pregnancy.
Common Arterial Trunk is a rare cardiac anomaly accounting for 1-2% of all congenital heart defects in newborns, and is characterized by a single arterial trunk that exits the heart and gives rise to the coronary, systemic and pulmonary circulatory vessels. It occurs in approximately 1 in 10,000 live births and is more commonly found in diabetic mothers. The aorta and main pulmonary artery originate from a common root and failure of separation results in a common arterial trunk with a common truncal valve. This common truncal valve can either be stenotic or insufficient and comprises four or more leaflets. Frequently, a common arterial trunk overrides a large ventricular septal defect [1].

Classification Systems
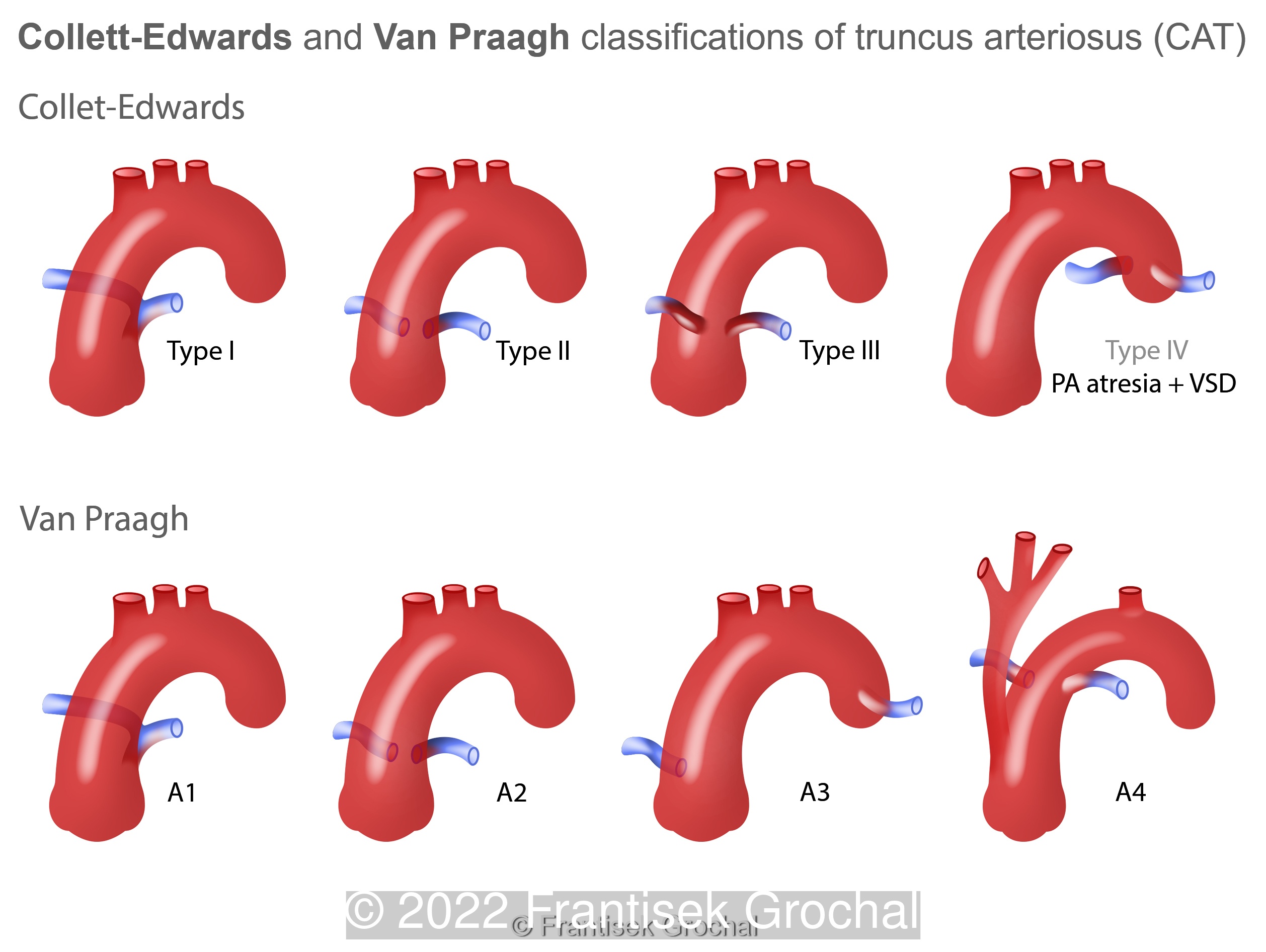
The Collet-Edwards system was developed in 1949 and describes the relationship between the pulmonary arteries and the common trunk (Image 10) [2].
- Type I: The main pulmonary artery is present and bifurcates into the left and right pulmonary arteries
- Type II: The right and left branches arise near each other from the posterolateral segment of the common trunk
- Type III: The right and left branches originate on the posterolateral segment of the common trunk but are more distant from each other.
- Type IV: The pulmonary arteries arise from the aortic arch or the descending aorta. This type is now categorized as a form of pulmonary atresia with a ventricular septal defect rather than a Common Arterial Trunk.
The Van Praagh system not only describes the location of the pulmonary arteries in relation to the common trunk, but also the development of the aortic arch and the presence of a patent ductus arteriosus (PDA). Each type may include a modifier “A” (with the presence of a VSD) or “B” (an intact ventricular septum) [2].
- Type 1: Similar to Collette and Edwards classification, the main pulmonary is present and bifurcates into the left and right pulmonary arteries.
- Type 2: The right and left pulmonary artery branches arise from the common arterial trunk.
- Type 3: One branch of the pulmonary artery, most often the right, arises from the common trunk and the other arises from a patent ductus arteriosus or the aorta.
- Type 4: The presence of aortic arch hypoplasia, coarctation or interrupted aortic arch occurs in approximately 1% of cases with Common Arterial Trunk. In these cases, a large patent ductus arteriosus is the primary blood supply to the lower body.
Associated anomalies are common in patients with Common Arterial Trunk. In two large European series from Amsterdam and Germany, genetic syndromes are found in 38-39%, most commonly chromosome 22q11.2 deletion syndrome. Cardiac anomalies were identified in approximately 29-37%, and extra-cardiac manifestations in 53-59% of patients. Only 27-39% had an isolated common arterial trunk [1,3].
Morbidity and mortality in patients with Common Arterial Trunk are high. In the Amsterdam series, the risk of fetal demise is 10% in continuing pregnancies, with an overall survival rate into childhood of 60% [3]. In reviewing the literature, van Nisselrooij et al found that the presence of additional anomalies is an important predictor for mortality, as genetic syndromes or extra-cardiac manifestations were found in 75% of non-survivors compared to 31% of survivors [3]. Additionally, premature birth contributes to mortality as none of the infants that delivered prematurely survived until corrective surgery could be performed. In patients with isolated Common Arterial Trunk, the presence of prenatal truncal valve regurgitation was associated with fetal and postnatal mortality. In continuing pregnancies with a prenatal diagnosis of Common Arterial Trunk, only 30% were alive without additional morbidity or developmental delay at 6 years of age [3].
As genetic syndromes and developmental delay are common in cases with Common Arterial Trunk, microarray analysis with sequential exome sequencing should be considered in order to offer better prenatal counselling [3].
References:
[1] Abel JS, Berg C, Geipel A, et al. Prenatal diagnosis, associated findings and postnatal outcome of fetuses with truncus arteriosus communis (TAC). Arch Gynecol Obstet. 2021 Dec;304(6):1455-1466
[2] Lai, W. W. (2009). Truncus arteriosus. In Echocardiography in pediatric and congenital heart disease: From fetus to adult (pp. 385-392). Chichester, UK: Wiley-Blackwell.
[3] van Nisselrooij AEL, Herling L, Clur SA, et al. The prognosis of common arterial trunk from a fetal perspective: A prenatal cohort study and systematic literature review. Prenat Diagn. 2021 May;41(6):754-765.
Discussion Board
Winners

Dianna Heidinger United States Sonographer

Javier Cortejoso Spain Physician
Danilo Feitosa Brazil Physician

Pawel Swietlicki Poland Physician

Fatih ULUC Turkey Physician
Umber Agarwal United Kingdom Maternal Fetal Medicine

Igor Yarchuk United States Sonographer

Andrii Averianov Ukraine Physician

Ana Ferrero Spain Physician

Alexandr Krasnov Ukraine Physician

Mayank Chowdhury India Physician
filiz halici öztürk Turkey Physician

Oskar Sylwestrzak Poland Physician

Vladimir Lemaire United States Physician

Tatiana Koipish Belarus Physician
Halil Mesut Turkey Physician
Miğraci Tosun Turkey Physician

Rushina Patel United States Sonographer
Caroline Reichert Garcia Brazil Physician

Suat İnce Turkey Physician

Elena Andreeva Russian Federation Physician
santosh shahare United States Physician

Muradiye YILDIRIM Turkey Physician

Ta Son Vo Viet Nam Physician

ALBANA CEREKJA Italy Physician

Selvanandhini Gopalasundaram India Physician

Murat Cagan Turkey Physician
gholamreza azizi Iran, Islamic Republic of Physician
Rasha Abo Almagd Egypt Physician

Ionut Valcea Romania Physician
LILY LI China Physician
Karin Tinnemeier Germany Physician

Abdullah Alnoman Canada Physician
Borisova Elena Russian Federation Physician

Kathrine Montagne United States Sonographer
Dr Praveen Kumar United States
Anna Zhampeissova Kazakhstan Physician

Haitham Baghlaf United States
Nadezhda ROMANENKO Russian Federation
Nina Dotsenko United States
Sowmya Mohan United States
corey nash United States
Michael Hussey United States Physician
Alexandra M United States

TATIANA VOLKOVA Kyrgyzstan Physician
SVETLANA Zhumazhanova United States
Amy Scholl United States